Thoracic endometriosis is a form of extra-pelvic or intraperitoneal endometriosis that occurs when lesions spread to the diaphragm and the lungs. Due to the variety of organs involved, it is one of the most complex forms of endometriosis to surgically treat. It can occur on the dome of the diaphragm, the lung parenchyma, visceral and parietal pleura, and even the tracheobronchial tree.
Thoracic endometriosis is particularly challenging to identify unless respiratory symptoms are clear and present. Many physicians fail to establish a correlation between thoracic symptoms and a woman’s menstrual cycle. Thoracic endometriosis can be the source of catamenial pneumothorax (pneumothorax development during menstruation), catamenial hemothorax (blood collection in the pleural space during menstruation), catamenial hemoptysis (coughing up blood during menstruation), and lung nodules.
Get a Second Opinion
Our endometriosis specialists are dedicated to providing patients with expert care. Whether you have been diagnosed or are looking to find a doctor, they are ready to help.Our office is located on 872 Fifth Avenue New York, NY 10065.
You may call us at (212) 988-1444 or have your case reviewed by clicking here.
About the thoracic cavity
The thoracic cavity or the chest cavity is the chamber of the body protected by the rib cage and associated skin, muscle, and tissue. It contains two highly vital organ systems. These are the respiratory system (lungs, bronchi, esophagus, etc.) and the cardiovascular system (the heart and its blood vessels). It begins with the esophagus, right around the base of the neck, and ends with the diaphragm. The diaphragm separates the thoracic cavity from the abdominal cavity. The central compartment of the thoracic cavity is the mediastinum.

What is thoracic endometriosis?
Thoracic endometriosis is when endometrial tissue occurs in or around the thoracic cavity. This can include the lungs and diaphragm. It is a complex and rare condition, and diagnosis is often late. This can lead to recurrent hospitalizations and other medical complications.
What areas of the thoracic cavity can endometriosis affect?
Thoracic endometriosis can affect any of the following regions:
- Lungs
- Pleura (the serous membranes that line the thoracic cavity and surround both lungs). The pleura has both an inner layer (visceral pleura) and an outer layer (parietal pleura). There is an intermembrane space in between the two (pleural space).
- Heart
- Pericardium (the membrane surrounding the heart, consisting of a fibrous outer layer, and inner double serous membrane).
- Diaphragm (the long sheet of internal skeletal muscle that extends to the bottom of the thoracic cavity). It plays a key role in breathing. It also separates the thoracic cavity from the abdominal cavity.
What is a pneumothorax and how does it relate to endometriosis?

Endometriosis lesions in the thoracic cavity are of particular concern due to their association with catamenial pneumothorax. When there is a small rupture in the lung, pneumothorax occurs. Here, air leaks out of the lungs into the space between it and the chest wall (pleural space). The high pressure this creates against the lung wall (visceral pleura) can, in turn, cause the lung to partially or totally collapse.
A pneumothorax can be related to a variety of different disorders. These include diseases of the respiratory airways (i.e. COPD and severe asthma) and lung infections such as severe pneumonia and tuberculosis. However, in patients with endometriosis or a family history of endometriosis, there is concern if pneumothorax is related to the menstrual periods. If a patient receives a diagnosis of pneumothorax, particularly repeatedly, it is important to check whether these symptoms coincide with the monthly menstrual cycle.
Pneumothorax is often marked by a total or partial collapse of the lung.
Why do doctors often fail to notice thoracic endometriosis?
The average physician can often misdiagnose endometriosis. This is especially so if lesions are in the thoracic cavity. Unless there is chest pain, difficulty breathing, or other clear respiratory symptoms, doctors will not suspect thoracic endometriosis. More importantly, when these symptoms do come up, rarely is a physician thinking of a possible thoracic endometriosis case. Instead, the doctor will only look to rule out cardiovascular and respiratory issues. However, doctors should not treat pneumothorax without considering its primary origin. In some cases, this can be the pelvis. When this goes unnoticed and in turn misdiagnosed, many of these patients do end up getting repeated thoracic surgeries without the patient or doctor knowing what is happening.
The important question to ask
It is indeed important, in cases of chest pain and shortness of breath, to rule out cardiovascular and respiratory disease first. However, it is also crucial that a physician considers the source of the symptoms. In cases where respiratory and cardiovascular tests are unremarkable, but there are repeated instances of pneumothorax, and particularly when there is a history or family history of endometriosis, doctors should suspect thoracic endometriosis. The key question is whether the clinical picture overlaps with the patient’s period. If a pneumothorax is recurrent and/or there is a relationship between the patient’s symptoms and the menstrual cycle, the cause may be of uterine origins, such as endometriosis.
Symptoms of thoracic endometriosis
The common symptoms of endometriosis can also occur in the case of thoracic endometriosis. But there are also five distinct clinical entities that are of particular concern for endometriosis in the thoracic cavity:
Catamenial pneumothorax
This is pneumothorax occurring in conjunction with a woman’s period. In other words, recurrent air leakage out of the lung and into the pleural space, with a particular association with one’s menstrual cycle. This should be of particular concern if a patient keeps having to go to the hospital with recurrent pneumothorax.
Catamenial hemothorax
A hemothorax is a collection of blood in the space between the outer lung and the chest wall (pleural space). Thus, a catamenial hemothorax is a hemothorax in conjunction with menstruation. Once again, this is of particular concern to endometriosis patients when there is a recurrent hemothorax with no known cardiovascular or respiratory cause.
Catamenial hemoptysis
Catamenial hemoptysis is the coughing up of blood or blood-stained mucus. It can be a common sign of many lung or respiratory infections. However, if this symptom is recurring around the time of menstruation, it could be yet another sign of the underlying cause of the symptoms or infection related to thoracic endometriosis.
Pulmonary nodules
These small single masses in the lungs, while benign, can be the cause of other symptoms above such as hemoptysis. However, it is also important to consider the etiology of the nodules themselves. Coupled with any of the symptoms above, these can point towards endometriosis.
Catamenial chest pain and/or shortness of breath
Intermittent chest pain or shortness of breath is often attributed to cardiovascular or respiratory diseases. However, if a patient’s symptoms are recurring monthly or specifically in sync with their menstrual cycle, it is important they alert their physician, as this can be a key clinical indication of thoracic endometriosis.
Diagnosis of thoracic endometriosis
Medical history and physical examination
In order to diagnose thoracic endometriosis, a gynecologist must be highly thorough and meticulous in their medical history taking, as well as in their physical examination. It is important for a patient to let their doctor know if they have a history of recurrent pneumothorax, intermittent chest pain, and shortness of breath during their menstrual cycle, and if they have endometriosis or a family history of the disease. In terms of physical examination, if a patient has tenderness upon a pelvic and/or rectovaginal exam, with symptoms including catamenial chest pain or shortness of breath, and history of pneumothorax, these are all signs that can point towards thoracic endometriosis and warrant thoracic cavity inspection.
Imaging testing
One of the common ways to diagnose pneumothorax is via a chest x-ray. Recurrent pneumothorax, particularly at the time of a woman’s period, is one of the key clinical indications of thoracic endometriosis. An endovaginal ultrasound is also critical. It can point towards endometriosis within the pelvic cavity, and thus the possible etiology of the catamenial symptoms themselves. A CT scan or MRI are also highly useful imaging tests that an endometriosis specialist may advise for further diagnostic testing.
Surgical diagnosis (laparoscopy and thoracoscopy)
Imaging tests and meticulous medical history taking can all point towards possible thoracic endometriosis. However, laparoscopic and thoracoscopic surgery are the primary ways to view lesions and confirm a diagnosis. Both are minimally invasive forms of surgery. They simply require small incisions, through which the surgeon inserts a camera (scope). The surgeon can then use excision clippers to cut out suspected endometriosis lesions, obtain a biopsy, and send it to a pathology lab for confirmation of diagnosis. Thus laparoscopic excision and thoracoscopic excision/resection are the gold standards for surgically diagnosing a patient with suspected thoracic endometriosis.
Treatment of thoracic endometriosis
Laparoscopy and thoracoscopy
Laparoscopic excision surgery is the gold standard for surgically treating endometriosis located in the pelvic and abdominal cavity. It removes lesions while preserving healthy surrounding tissue. It also allows the surgeon to obtain a biopsy sample that they send to pathology to confirm a diagnosis. This is also a minimally invasive surgery. It uses minimal electricity and heat, ensuring quicker recovery time and relief of symptoms. It is important to assess the pelvic and abdominal cavity for suspected thoracic endometriosis cases, as this can provide insight into the cause of the patient’s respiratory symptoms.
Suspected endometriosis lesions in the thoracic cavity can also be removed by minimally invasive surgery. Excision of these lesions is done via video-assisted thoracoscopic surgery (VATs). The surgeon will either excise these lesions individually or will have to resect part of the organ or membrane that the disease affects.
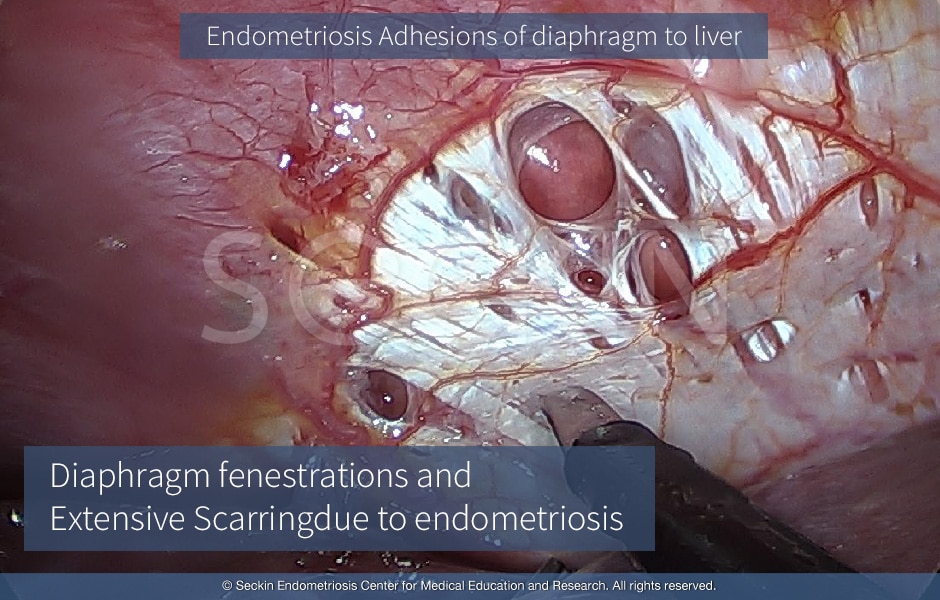
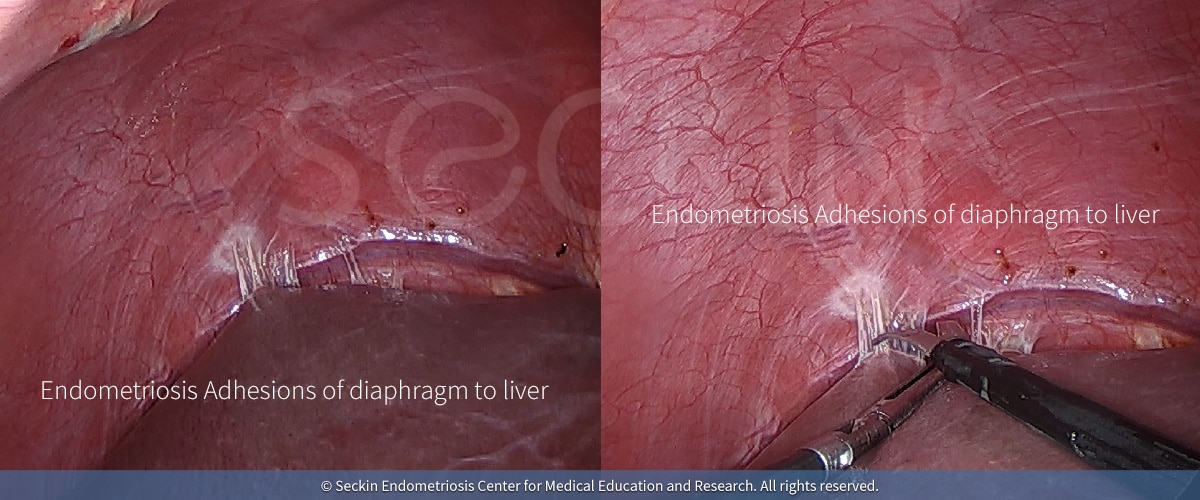
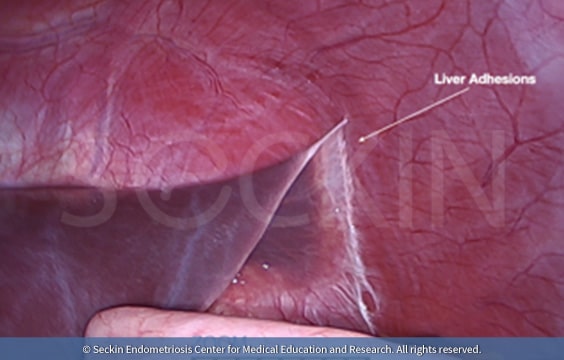
Why do surgeons have difficulty visualizing thoracic endometriosis?
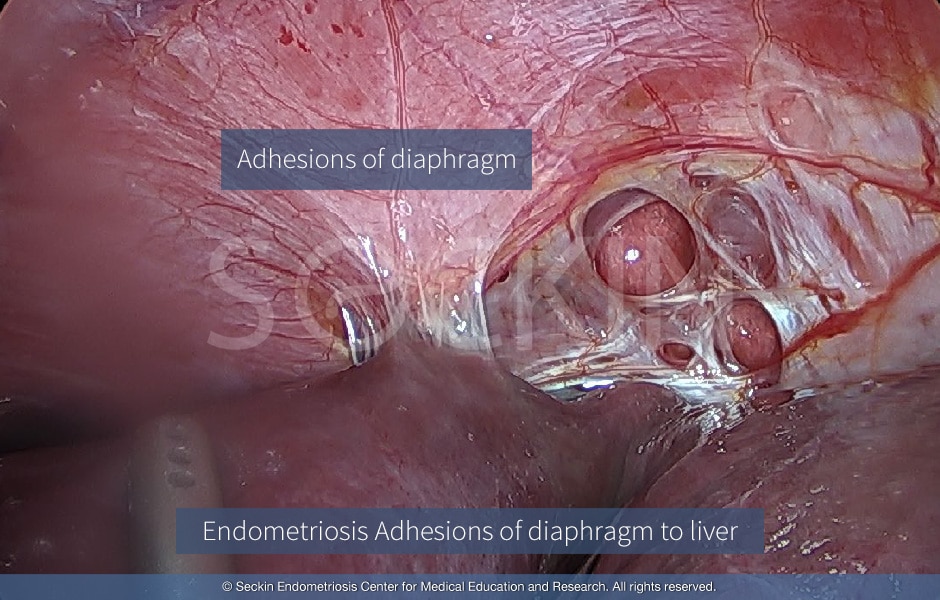
Thoracic endometriosis is typically easier to recognize on the dome of the right side of the diaphragm. The caveat here is that visualizing in direct view does not rule out endometriosis lesions that the curve of the liver may obscure. Therefore, doctors must use the technique of the 30-degree scope and look behind the liver by pressing down on it and examining the dome of the diaphragm. There may be lesions on the diaphragm that can reflect the pericardium, even on the right side. Therefore it is crucial to perform surgery alongside a thoracic surgeon in order to properly treat these lesions. The left side of the diaphragm can be observed in the same way. However, if one reaches the pericardium, it is imperative to have a thoracic surgeon on-site.
Our approach
Thoracic endometriosis remains a challenge for clinicians. When chest pain, shortness of breath, hemothorax, or recurrent pneumothorax occurs in women of reproductive age, a diagnosis of diaphragmatic or thoracic endometriosis must be considered. There is a strong association between thoracic endometriosis and severe pelvic endometriosis and infertility. Therefore, it is necessary to conduct a thorough evaluation of the pelvis in patients with thoracic endometriosis to rule out possible pelvic endometriotic lesions. In many of these patients who are treated with VATs by thoracic surgeons, the involvement of an experienced gynecologist is essential. Patients who desire to conceive should undergo excision of any pelvic endometriotic lesions.
The dual compartment approach
Up to 80% of women with thoracic endometriosis also have endometriosis lesions in the abdominal/pelvic cavity. Yet the surgical treatment of the disease is typically performed in separate procedures. Therefore, we believe that when an endometriosis patient shows clinical signs of thoracic endometriosis, they need to have what we call a dual compartment approach. This is a combination of both minimally invasive laparoscopic surgery and VATs. In other words, a thoracoscopic surgeon should look through the thoracic cavity, while the gynecological surgeon looks through the abdominal and pelvic cavity for any signs of endometriosis lesions. The positive endometriosis findings within the pelvis in patients with a history of recurrent pneumothorax is an indication for thoracoscopic inspection.
Thorough laparoscopic excision surgery for thoracic endometriosis
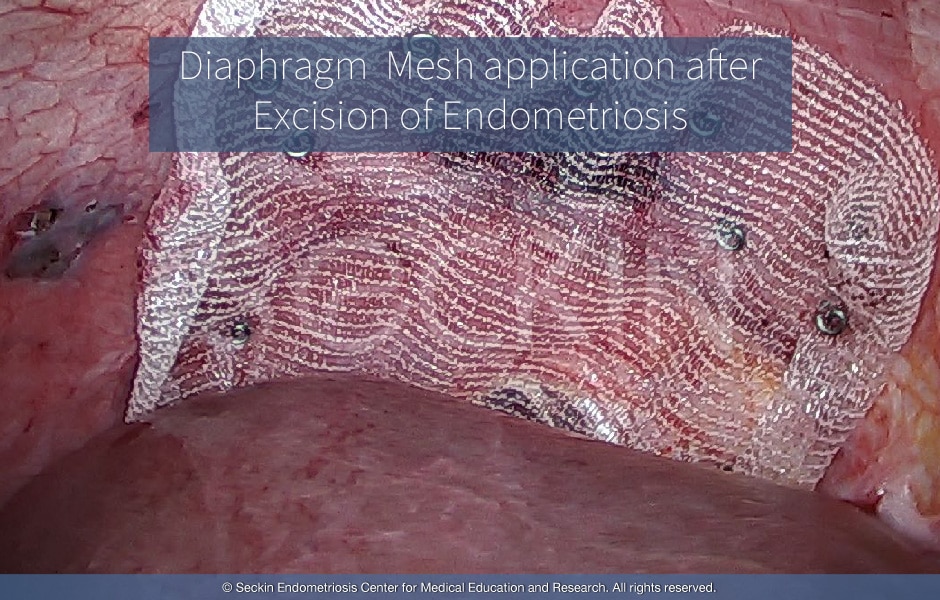
In addition to proper minimally invasive visualization of both the abdominal/pelvic and thoracic cavity, we stress the importance of properly removing the endometriosis itself. Lesions can be taken out via laparoscopy and suture. However, if there are lesions within the thoracic cavity, thoracoscopy is necessary and the lesions can be removed by a staple. We have done this in our practice for many years. We have great experience in suturing transmurally through the full thickness of the diaphragm. There are even cases where we may apply a mesh covering, even when there is no obvious hole in the diaphragm, but the defects are visible and large, in order to prevent further pneumothorax. This procedure is often performed on patients with recurrent catamenial pneumothorax, along with possible lobectomies, partial lobectomies, and lung resection procedures.
The importance of assessing the diaphragm
Finally, in every laparoscopic examination, we ask specific questions to ensure that there is no history of pneumothorax. If there is, we believe that one of the first things that need to be assessed upon surgery, along with the liver and upper abdomen, is the status of the diaphragm.
If you feel you are suffering from recurrent chest pain and/or shortness of breath, are having recurrent pneumothorax, and have a family history of endometriosis, find a physician that you both need and deserve to diagnose such a complex disease.
Patient story
The New York Times featured the care of an anonymous patient at the Seckin Endometriosis Center who received a diagnosis of thoracic endometriosis. Even after undergoing pleurodesis (mechanical attachment of the lung to its pleural lining) by a thoracic surgeon, the patient continued to suffer from multiple episodes of catamenial pneumothorax. It was not until surgeons at the Seckin Endometriosis Center and the patient’s thoracic surgeon performed a dual compartment approach that the patient finally received a proper diagnosis and surgical treatment.
You can read more stories of patients with thoracic endometriosis, and other types of endometriosis, in our testimonial section.
Get a Second Opinion
Our endometriosis specialists are dedicated to providing patients with expert care. Whether you have been diagnosed or are looking to find a doctor, they are ready to help.Our office is located on 872 Fifth Avenue New York, NY 10065.
You may call us at (646) 960-3080 or have your case reviewed by clicking here.

Dr. Seckin is an endometriosis specialist and women’s reproductive health advocate. He has been in private practice for over 30 years at Lenox Hill Hospital with a team of highly skilled personnel.
Dr. Seckin specializes in advanced laparoscopic procedures and is recognized for his expertise in complex cases of deep infiltrating endometriosis of the pelvis. He is particularly dedicated to performing fertility-preserving surgeries on cases involving the ovaries.
He has developed patented surgical techniques, most notably the “Aqua Blue Excision” technique for a better visualization of endometriosis lesions. His surgical techniques are based on precision and microsurgery, emphasizing organ and fertility preservation, and adhesion and pain prevention.
Dr. Seckin is considered a pioneer and advocate in the field of endometriosis.